Many people don’t understand what migraine disease is, how it can be treated and how it affects people. For example, many people are unaware that migraine is a hereditary condition that often runs through families.
Common myths about migraine disease include that migraine is a women’s problem, eliminating certain foods from your diet will stop migraine attacks, or headache medication will cure migraine. However, many men also get migraine, diet is complicated (for example, craving chocolate and cheese are often part of the early stage of a migraine attack, rather than causing it; caffeine can help treat a migraine attack, but caffeine withdrawal can trigger one) and there is no cure for migraine, despite what some people claim – although it can be managed successfully.
The most common myth, that migraine is ‘just a headache’, can lead to misunderstandings about the severity and impact of migraine disease. The effects of a migraine attack can last for hours to days, beyond the headache stage, and other symptoms of a migraine attack can be as debilitating as the headache, including nausea and vomiting, visual disturbances, light and sound sensitivity, brain fog, speech difficulties, fatigue and mood changes.
It’s not only the general public who don’t have a good understanding of migraine disease. Health professionals may not know how to distinguish migraine from other headache conditions, or be aware of the best management options. Dr Katy Munro, a headache specialist GP in the UK says, “Many doctors lack training in migraine diagnosis and treatment” and Dr Tissa Wijeratne, a neurologist in Australia, says that, “migraine is … the least respected and worst managed medical disorder worldwide”.
Without a broad and widespread understanding about migraine disease among society, health professionals, employers, educators and others, people with migraine in New Zealand can struggle to get diagnosed, and get the treatment and support they need to manage migraine in the best possible way.
People with migraine in Aotearoa New Zealand often face difficulties in accessing neurologists or other headache specialists, especially if they can’t afford private health care. There is a shortage of health professionals with specialised knowledge about migraine. For example, the Australia and New Zealand Headache Society (ANZHS) keeps a directory of clinicians with an interest in headache. As of 2026, there were only four in New Zealand.
We know there are many more neurologists and specialists who are interested in migraine disease, but it can be difficult to find them.
The proportion of a population who has a specific disease in a given time period is known as ‘prevalence’. The most recent estimates of the prevalence of migraine in New Zealand come from the 2023/24 New Zealand Health Survey (NZHS) and the Global Burden of Disease 2023 study.
The NZHS found that 17% of adults (aged 15 years or older) reported having been diagnosed with migraine by a doctor (11% of men and 23% of women). The survey also found that 15% of adults had symptoms consistent with migraine in the last 3 months. Of those with symptoms, only around half had been diagnosed with migraine by a doctor.
The Global Burden of Disease 2023 study also estimated that around 15% of people in New Zealand had migraine (12% of males and 18% of women), which is similar to global estimates. This was a measure of annual prevalence (how many people experienced the disease in one year). This equated to over 730,000 people in 2023 in New Zealand and over a billion people worldwide.
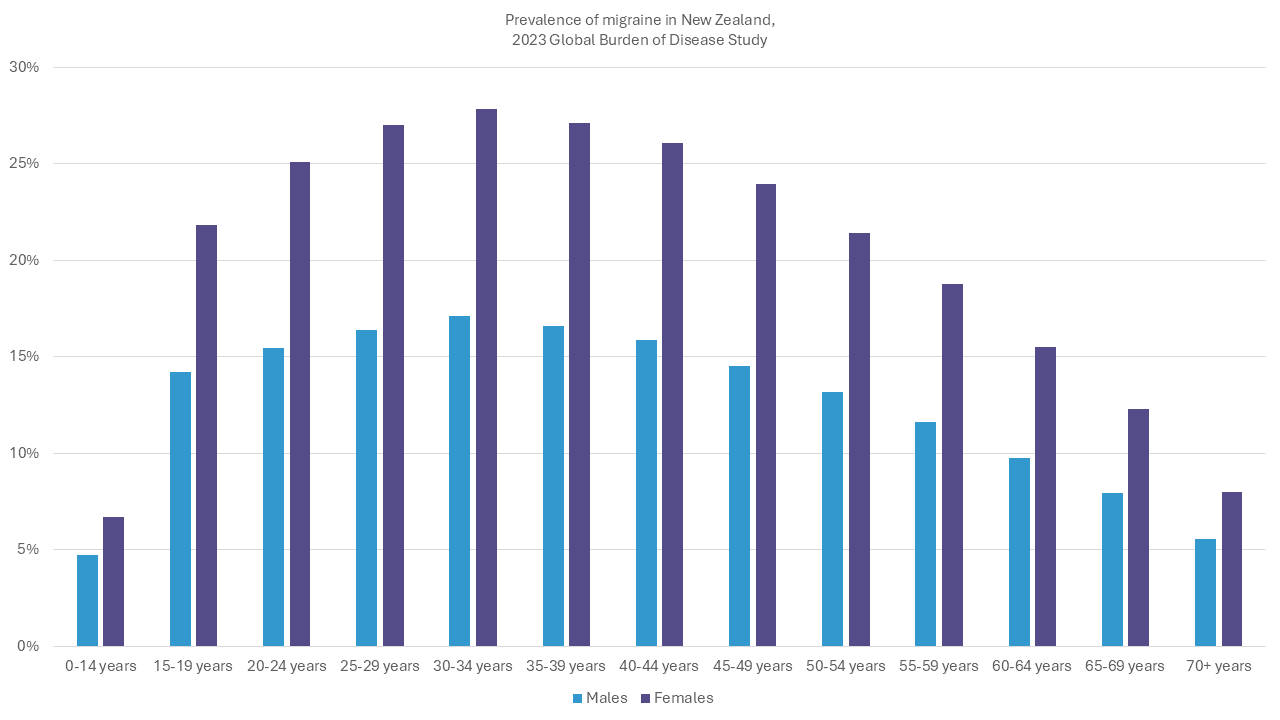
Based on Global Burden of Disease 2023 data, available at https://vizhub.healthdata.org/gbd-results/, accessed June 2024
In New Zealand, migraine disease is more common than many other conditions that cause pain or affect the brain and is more prevalent than diabetes, epilepsy and stroke combined.
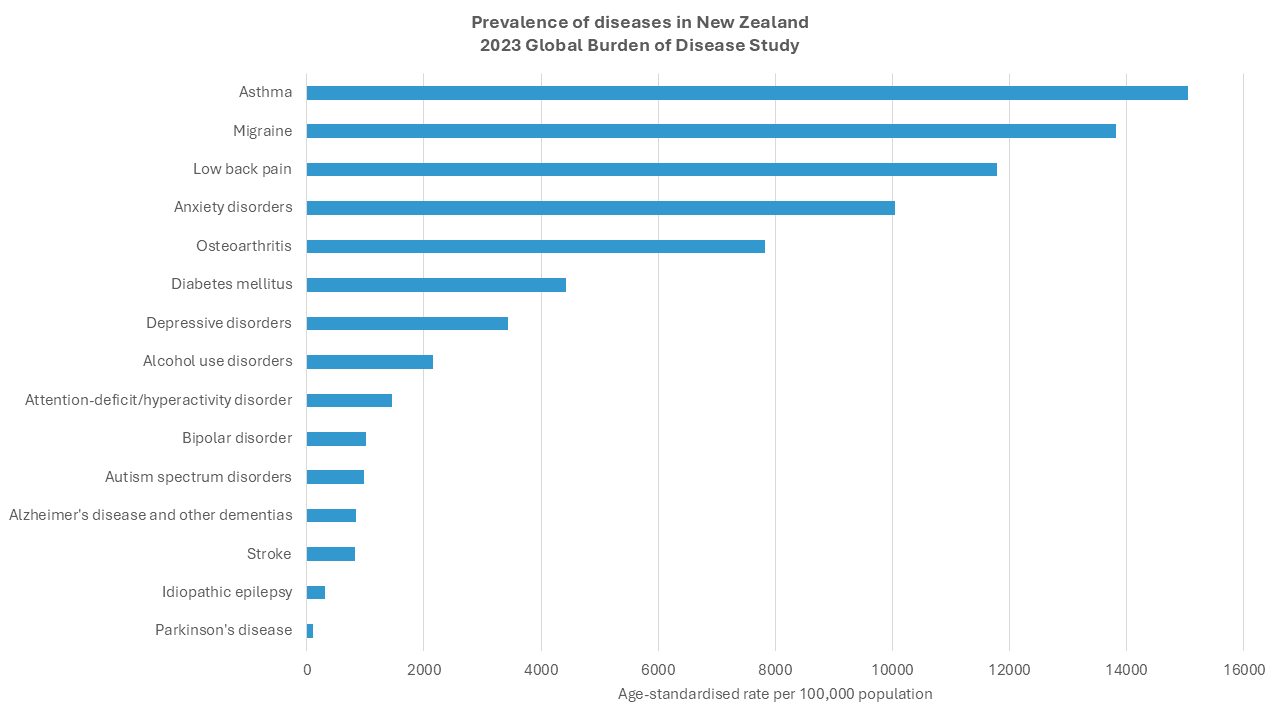
Based on Global Burden of Disease 2023 data, available at https://vizhub.healthdata.org/gbd-results/, accessed October 2025
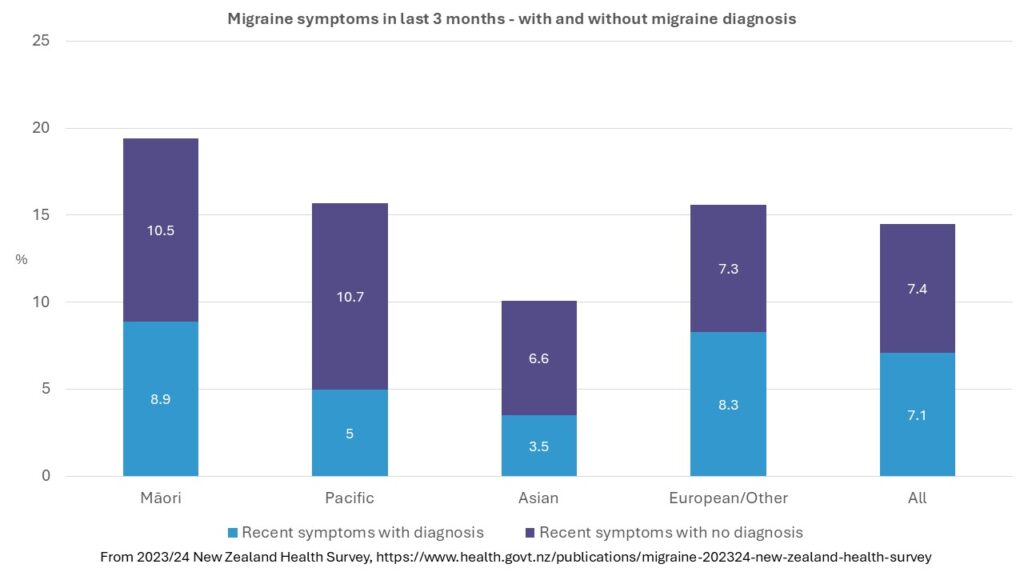
From the 2023/24 New Zealand Health Survey (NZHS), 17% of Māori had been diagnosed with migraine by a doctor but around 20% had experienced migraine symptoms in the last 3 months. Māori were not only more likely than non-Māori to experience migraine symptoms but also more likely to have symptoms but not have a migraine diagnosis.
For Pacific people, only 9% had a migraine diagnosis but 16% experienced migraine symptoms in the last 3 months. Pacific people were significantly less likely than non-Pacific to be diagnosed with migraine.
More research is underway to explore the reasons for these disparities and how they can be addressed. For other inequalities in health outcomes for Māori and Pacific people in Aotearoa, these are often related to differences in access to health care, experiences of stigma and discrimination and other factors. It’s probable that migraine is not only less well recognised and managed in Māori and Pacific people, but the impact is greater.
Despite a growing awareness of the impact of migraine globally, and the development of migraine-specific treatments, we know very little about the burden of migraine disease in Aotearoa.
The Health Research Council (HRC) is the primary source of Government funding for general health research and spends millions of dollars each year. The HRC has an online library of research projects that it has funded over the past ten years. A search in 2026 found just two projects with relevance to migraine, one worth $30,000 scoping out a migraine cost of illness study and one worth $500,000 looking for a new target to treat neurological pain, with a main focus on low back pain. By contrast, there were 54 studies on stroke, 38 on dementia and 20 on Parkinson’s disease.
From the charitable sector, the Neurological Foundation is New Zealand’s leading charity that supports neurological research. The Neurological Foundation’s 50th anniversary publication in 2021 reported having allocated only $147,000 to migraine, headache and tinnitus research (combined) in 50 years, from a total funding pool of nearly $52 million. This is despite migraine causing the second highest burden of disability in the world, in global rankings of disease.
Since then, the Neurological Foundation has funded several migraine-specific projects, including in-depth analysis of the NZ Health survey and development of a migraine workplace programme.
In 2023, Professor Debbie Hay, Department of Pharmacology and Toxicology, University of Otago, was awarded $941,000 from the Marsden Fund for research into CGRP receptors and their relationship to migraine disease.
We have also undertaken our own research, beginning with our 2022 Migraine in Aotearoa New Zealand survey.
We need more research like this, to raise awareness of the impact of migraine and to investigate better ways to diagnosis and treat migraine effectively.